
Enjoy the audio preview version of this article—perfect for listening on the go.
This article first appeared in the November/December 2008 issue.
“We know we must not run away from suffering.
The truth of suffering contains the truth of emancipation.”
—Thich Nhat Hanh
Thursday
It’s hard to believe that I’m on a plane going to Rwanda. Nearly two years ago, we were invited here by a community-based organization to teach a group of counselors in Kigali about a somatic treatment for trauma and meet with genocide perpetrators in prison. Now that four of us—two from my organization, Trauma Resource Institute—are actually in transit, I’m wondering how one possibly prepares to go into a country that’s experienced such horrors.
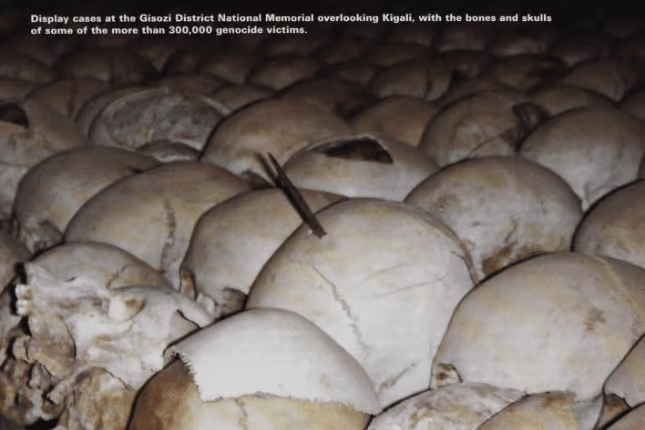
In the spring of 1994, ethnic tensions between the Hutus and Tutsis in Rwanda erupted into a massive genocide. More than 70 percent of the country’s Tutsis were murdered—between 800,000 and 1 million men, women, and children in a three-month period—making it the most ferocious genocide in recorded history. On command of the Interahamwe, the government-supported Hutu paramilitia organization, neighbors killed neighbors, friends killed former friends and their children, and trusted authority figures like priests and teachers turned on the people who looked to them for safety. Now, 14 years later, almost half of Rwanda’s population is younger than 15. While the 1994 slaughter-by-machete was going on, many Americans were glued to their television sets watching the O. J. Simpson murder trial.
In February 2005, I was a member of a team from the Foundation for Human Enrichment who went to southern Thailand after the tsunami to use Somatic Experiencing (SE) to help the traumatized survivors (see Psychotherapy Networker, November/December 2005). After that experience, another teammate and I formed the Trauma Resource Institute (TRI), a nonprofit organization that offers treatment and training in a brief-stabilization model we call the Trauma Resiliency Model (TRM), inspired by SE. A central part of TRI’s mission is to provide affordable, three-day training to clinicians who work with underserved, at-risk populations to build local capacity nationally and internationally. We’re on our way to Rwanda to conduct TRM training sessions.
Saturday
We’re in Kigali, the capital of Rwanda, in central Africa. All of our luggage has been lost en route from London, so we set out with our driver-translator, Peter, to buy necessities.
Kigali, a bustling city of more than 600,000, has a mix of dirt and paved roads, tall buildings, modern hotels, and small, tin-roofed houses, all jammed together among numerous hills. As we drive through the streets, Peter points out places where large-scale massacres occurred. He gives us tips about what not to do while we’re here: don’t photograph anything military, don’t ask about anyone’s ethnic identity, don’t talk politics, don’t ask too many questions. At dinner later, after requesting a table in a quiet, out-of-the-way corner of the restaurant, he goes into more detail in a hushed voice. He’s a Tutsi and bears the scars of his own experience from the genocide.
Back in my room, I feel less safe than I did upon arrival, despite, or maybe because of, the armed guard employed by the guesthouse. As I write and read in my room, the blare of a violent television show playing in the reception area cuts through the night. I notice some fear at being here. Even though the genocide happened 14 years ago, in some ways it feels quite present.
Monday
We’re going to the prison on Wednesday and hope eventually to develop a program that trains selected prisoners to provide TRM to other prisoners. This trip is a first step, an opportunity to begin developing relationships at the prison, and to learn about the needs of the prisoners, called genocidaires, who perpetrated or are accused of perpetrating the genocide.
There’s a strong emphasis in Rwanda on a truth-and-reconciliation process, somewhat similar to the model in South Africa after apartheid. I’ve been told, however, that many prisoners are unable or unwilling to take responsibility for their acts, and therefore can’t participate fully in efforts to reunify the country. I suspect that many of the genocidaires, as a result of what they did and saw, must be in a physiological state of immobilization, or in SE parlance, a “freeze.” Without some way of coming out of the frozen emotional state, their healing and rehabilitation will be difficult.
Wednesday
All the years that I was working in my private practice in Washington, D.C., I never dreamed I’d one day be walking hand in hand with an African social worker down a dusty path into a Rwandan prison. But today, that’s exactly what I’m doing. My mind is filled with questions: what’s a white, middle-class woman like me doing here? what’ll it be like to sit with genocide perpetrators? do I have anything to offer in a country so torn apart by tragedy?
As the other members of my team and I approach the Kigali prison building, I look behind me. Following closely are perhaps 50 people, mostly women, in colorful dress. They carry baskets of food on their heads and satchels with more food for the prisoners they’re visiting. It’s Wednesday, the main visiting day. The visitors sit on long benches just outside the main building.
When a whistle blows, a group of pink-uniformed prisoners hurries out and sits on another long bench across from their respective family members. Talk is rushed because each group has only about seven minutes before the whistle blows again and the family members must leave to be replaced by another group, and then another and another. There are about 6,000 prisoners in this prison, all of whom are accused of committing the severest crimes, such as planning the genocide or murdering many people. Some have confessed; others haven’t. Some have been sentenced; most haven’t.
It’s been arranged that we’ll meet with a group of genocidaires. I’m nervous when we join the assembled group of men. The language barrier strongly hinders most efforts to put everyone at ease. We have a translator, but many of the men talk at the same time, and then a prisoner who speaks English accuses the translator of not translating accurately what they’re saying.
We soon learn that the prisoners were never told who we were or why they were part of this group. One man explains that many factions of prisoners who don’t usually speak to each other are there, and nobody feels safe talking openly. I’m impressed that the men feel at least comfortable enough to speak up about this, and we offer to meet with them in small groups of their own choosing.
A teammate and I later meet with a group of three—two brothers and their friend. All three have confessed to their crimes, but after 13 years in prison, only one of them has been sentenced. Prisoners who’ve been sentenced wear orange uniforms. We see few of these, despite the time that’s elapsed since the genocide. The three men, like my own children, are in their mid-thirties.
One of the men, exactly my son’s age, is a Tutsi who killed his entire family in exchange for his own life. The brothers say he’s never been the same, and as we talk with him, his eyes fill with tears. We show the men how to do a simple grounding exercise in which they sense their feet on the floor and their backs supported by the wall. Then we ask them to describe something that gives each of them pleasure and sense where they feel it in their bodies. I’m relieved to see that the sensory tracking seems to help the prisoners feel more balanced, especially the one in distress. I see the tension leave his face, his hands relax, and a ghost of a smile appears on his lips. This brief demonstration of TRM gives me hope that we may have something to offer here.
I know that some of the genocidaires in this prison may be beyond rehabilitation or may not want to change, but I’m startled by how warmly I feel toward these young men. I try to keep imagining being at the other end of their machetes during the killings to keep myself alert to what they’ve done and guard against being manipulated, but all I feel is their humanity. This confuses me. How can good people turn into mass murderers?
Phillip Zimbardo, the designer of the Stanford University prison experiment, has spent his career studying the question of evil. In his book The Lucifer Effect, he contends that, in toxic settings, external factors can override individuals’ internal dispositions. He believes that the line between good and evil, considered by some to be absolute, is actually permeable.
Zimbardo emphasizes that his theory that evil comes from “a bad barrel” rather than “a bad apple” doesn’t excuse crimes or suggest that people don’t have to be held accountable for what they do, but he thinks we hold a false belief that good is separate from evil, when, in reality, good and evil are intertwined potentials, and either of them can emerge in any of us, depending on the context. Zimbardo’s book helps me understand my unexpected response to the genocidaires.
After our morning of interviews with prisoners, we’re invited to attend a fellowship gathering. To our surprise and embarrassment, we’re led into an auditorium of more than 400 prisoners, including about 100 women (a few holding babies in pink uniforms), and asked to sit on a stage along with a few prisoners and the fellowship ministers. The prisoners are singing beautiful gospel songs. Suddenly, a large group from the first few rows gets up and begins dancing energetically. I love to dance and find it hard to stay in my chair. Finally, I can stand it no longer and encourage my teammates to join me in getting off the stage. The prisoners are delighted and dance even more enthusiastically as we join them. In no time, we’re all sweating together.
When the dancing is over, we sit down with the prisoners on the long benches. I’m with the women—one white face, no pink uniform. I’m given a baby to hold, and I turn her to face the stage, so she won’t be afraid of my white skin. I feel the warmth of these women as they shyly smile at me and then look away quickly.
I’m aware of the strong pull to do more than is realistic during this trip. One of the prisoners says to one of the team members, “Now we’ve sung and danced with you, you need to come back and work with us.” He means this week. When my teammate says we’ll be back with more people, but not for a few months, the man says, “We don’t want more people. Now we know your warmth, and we trust you.” This conversation tugs at each of us. This stage of a project, when the time seems way too short to address the enormous needs we see, is especially hard.
Thursday
I awaken with some nervous flutters, listening to the sound of Muslim prayers over a loudspeaker. I’ve been imagining and preparing this training day for months, and here it is. There were many stories after the tsunami of well-intended Westerners rushing in to help, doing some type of treatment, and then rushing off without training any locals to carry on the work. I call this the hit-and-run approach to emergency intervention. Others have called it being a “disaster tourist.” To counterbalance this tendency toward short-term relief activities, we vowed when we set up our nonprofit that we’d focus on enhancing the capacity of local communities to incorporate somatic interventions into their own ways of working.
The training materials we brought include PowerPoint slides and—just in case there’s no electricity—large laminated posters highlighting the key points of our model. Before leaving home, we had our English texts translated into French, which many Rwandans speak. When we put up the posters, we find that there are some glaringly poor translations, which generates great amusement among the trainees. For example, a poster about ways to observe the activation of the nervous system is supposed to say “pupils dilate.” Instead, the French version means “students dilate.” These glitches help us all enjoy the humor of trying to share information across cultures.
We’re having the training translated into multiple languages. Many of the participants request that the translators use Kinyarwanda, the country’s indigenous language, while others want to learn in French. So our stalwart translators do both, sometimes translating questions and observations from the participants into English.
A key aspect of a somatic intervention is tracking bodily sensations. As we begin to show and discuss the skill of “tracking,” a participant tells us that there are no sensation words in Kinyarwanda. We’re told that the concept of feeling and sensation are much more similar in Rwanda than they are in the West. This poses quite a challenge, but several of the participants speak English and help us explain the language of sensation. One participant offers, “The smell of dead bodies is a sensation.” A member of our team pantomimes various other sensations, such as what it’s like to touch a hot stove or to have your heart pound during a fight with someone, which are greeted approvingly.
Because the translation process gets overwhelming in a large group, we break into smaller groups to do case demonstrations. We invite the participants to play the role of a client or work with material from their own lives. Many of our Rwandan participants choose to play their clients, which seems to give them a needed sense of personal privacy and helps insure that they’ll learn how to apply TRM to their challenging cases.
One counselor describes the sensation of having a machete slash on the crown of her head that she’s experienced since the genocide, even though she was never slashed. In my work with her, I have her sense just the edge of the sensation of the slash and alternate that with sensations in a part of her body that feel more comfortable, or at least neutral. After transfers of focused awareness between the trauma sensation of the slash and the calmer feelings in her chest, she reports that the slash sensations are no longer there.
I didn’t need to challenge her feeling that she had a slash on her head or ask why she thought she had one. I merely worked with the sensations as she tracked them in her body. At the end of the work, she described feeling warm on the top of her head and experiencing a trembling in her arms. We consider this type of discharge to be an indication that the blocked traumatic energy is being released. When I checked with her the next day, she said the slash sensations hadn’t returned.
Friday
The second day of training is much easier! The participants are more relaxed, and so are we. A counselor starts the day by having everyone stand in a circle. Each person speaks one word that describes how she or he is feeling. Then the next two people go into the center of the circle and act it out. Most of the descriptions are of pain or discomfort, but when two people go into the center to act out the pain of headaches and stomachaches (often signs of trauma), they do so with such exaggerated, melodramatic movements that everyone laughs uproariously.
In our training, we use animal videos to illustrate defensive responses. The participants love the videos and seem to understand the biological basis of these responses—in both animals and humans. We can see the increasing familiarity with somatic interventions as participants offer their own examples of the skills we’re teaching.
During one break, I see a translator engaged with three participants in a friendly argument about whether asking a patient to open her eyes during a session is “titration” or “pendulation.” I love watching them debate the characteristics of each skill and seeing the translator’s increasing comfort with the somatic work.
We spend a lot of time in practice groups today. The cases are intense and dramatic, since they deal with the postgenocide symptoms and behaviors of the counselors’ patients. Untreated trauma often manifests as violence, and there are stories of domestic violence, of clients who feel forsaken by God, and of clients coming into the counselors’ offices and needing to sleep for the entire session. Working somatically helps create a sense of manageability, since the client’s trauma story doesn’t need to be told, or at least told in great detail, because it “lives” in the body, and we can show the trainees how to work with the body to discharge the trauma.
The training ends with round after round of photo-snapping. There’s camaraderie among the participants and with us. One woman, a psychology student, slips a note into my hand thanking me for my “care and responsibility” and then asking if I’ll stay in Rwanda and be her friend and aunt. Her note feels like such a blessing to me. There’s no question that each of us on the team has learned as much as we offered.
Postscript
It’s now eight months since I was in Rwanda, and we’re actively raising funds for continuation of the prison project. I’ll carry the lessons I learned there for the rest of my life. Working at the most fundamental level of biological programming strips things down to the basic responses to trauma—the place we all share simply because we’re human.
Having come face-to-face with what many would consider the very heart of darkness, I’ve had plenty of opportunity to reflect on the concept of good and evil. I’ll never forget the experience of looking into the eyes of the genocidaires I interviewed and seeing, not evil, but bewilderment, anguish, and even gentleness.
As I write this, I imagine people reading this thinking: “What a typical do-gooder Westerner! If these genocidaires are so gentle, how did they slaughter hundreds of people?” But the reality in Rwanda is that one day these prisoners will go back to their villages. What chance do they have for reintegration without programs that help heal their trauma, so that they can accept responsibility for the horror they perpetrated and find a way to reenter the human community?
When I try to make sense of what took place in Rwanda, I’m reminded of something Alison Des Forges of Human Rights Watch wrote:
The simplified accounts of genocide allow distance between us and the perpetrators of genocide. They are so evil we couldn’t ever see ourselves doing the same thing. But if you consider the terrible pressure under which people were operating, you are forced to look at the situation and say, “What would I have done?” Sometimes the answer is not encouraging.
Photo by the author

Laurie Leitch
Laurie Leitch, PhD, is cofound and codirector of development and evaluation for the Resource Institute, which offers training in the brief stabilization model Trauma Trauma Resiliency Model First Aide. She’s the director of research for The Foundation for Human Enrichment.





