

Enjoy the audio preview version of this article—perfect for listening on the go.
Looking today at the cover of the first issue of this magazine from January 1982—when the magazine was called The Family Therapy NetWorker—is a little like unearthing a miraculously preserved papyrus manuscript from an ancient civilization, long superseded by other, more technically advanced, societies. Printed on what has the appearance of butcher paper (not the slick, shiny pages you’re holding now), with a black and white drawing of Milton Erickson on the cover, it’s 40 pages long (including front and back covers) with a grand total of six photos (also black and white) and one quite crude cartoon illustration. Edited on a typewriter in my basement in Tyson’s Corner, Virginia, it had 300 subscribers from its earlier incarnation as a mimeographed newsletter jauntily titled The Family Shtick. (Remember mimeograph? Of course not—you’re not that old!) In those days, nobody I knew had computers and nothing in our little publishing world was digitized. Pages were “laid out” by hand—photos and galleys waxed and pasted onto their meticulously measured spaces on large, heavy sheets—and then couriered over to the printer.
I was still so mired in the early 19th century that I’d never learned to type, so I had to hand-write my “Letters from the Editor” and articles, schlep the drafts to a professional typist (a 15-minute drive), then retrieve them, mark them up, and return them to be retyped on her IBM Selectric. However technically primitive the system and I were by today’s standards, it somehow all seemed to work. By the end of 1982—six issues later—our circulation had grown fourfold to 1,700, and by 1986, it was more than 18,000. That spring, when attendance at the ninth Networker Symposium reached 2,000, we finally had enough money to splurge on four-color covers. No father of a newborn ever felt more pride than I did when I first cast eyes on what finally looked like a real magazine, rather than a glorified pamphlet.
But whatever its appearance, it was always intended as a magazine—not a journal gathering dust on a library shelf. We wanted to produce something that people would actually read, something that conveyed a bit of the compelling drama, the sheer juiciness of what therapists experienced, day to day, case after case. We assumed that spending 25 or 30 hours a week seeing clients didn’t exhaust our readers’ curiosity (not unmixed with a tinge of voyeurism) about people—not just the people who went for therapy, but the people who treated them. It was, and still is, our apparently revolutionary belief that therapists are human, too, and that the line between personal and professional, between the self of the therapist and the clinical approach being practiced, is often thin, sometimes vanishingly so.
Movers and Shakers
Only a few years before the Networker was first launched, the entire family therapy literature hardly contained more than a handful of volumes, books that made up in grand claims what they lacked in sheer numbers. Authors at that time were especially partial to the phrase “paradigm shift” to describe how family therapy had moved beyond the hermetically sealed world of the individual psyche to recognizing the broader context of intimate human interaction.
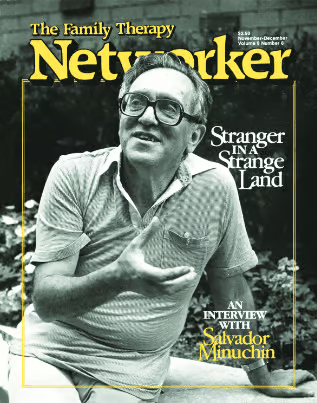
To be sure, the Networker also beat the drum for the game-changing potential of the “systems perspective” and published plenty of articles about the craft and theory of family therapy, but what drew people to us in those early days was probably less intellectually exalted—our unabashed fascination with the colorful personalities attracting such attention on the family therapy workshop circuit. During our early years, we became known as a kind of People magazine of the field, specializing in revealing interviews and profiles of the profession’s superstars—Salvador Minuchin, Carl Whitaker, Virginia Satir, Murray Bowen, Jay Haley, Mara Selvini Palazzoli, and others. Unlike traditional psychodynamic therapists, who kept a modest profile, these showstoppers commanded—even invited—a kind of hero worship and loyalty that, more than anything, explained the burgeoning field’s popularity.
Despite their theoretical and clinical differences, what this entertaining group of iconoclasts shared was a certitude that they could detect with fMRI-like precision the soft, pulsing, inner reality of the families they treated and rapidly transform it with a confidence that would be hard to find among the more cautious clinicians of today. Most of them rejected standard psychotherapies as irrelevant, secondhand knowledge about human interactions—barren textbook descriptions—that could never convey the direct, ever-shifting experience of therapy in the flesh that they were offering their workshop audiences. These movers and shakers showed little interest in the lumbering progress of therapy research, nor much in theory, except what was needed to propel the real action, which was making something striking and original happen in the therapy room. They were the action heroes of therapy, demonstrating a flair and sure-footedness that mere mortal therapists found dazzling. After 100 years of reserved, cerebral psychodynamic types, suddenly, our profession was home to a cast of riveting performers, each of whom attracted a following among the legions of baby boomers entering the field and looking for a role model to guide their development.
In the hierarchical professional culture of the early ’80s, it was expected that clinical wisdom would be passed down from the omniscient-seeming elders to the masses of far less self-assured practitioners. Therapists defined themselves by a fierce allegiance to a particular school of therapy, as if looking for a theology that would give definitive answers to all the ambiguities they had to face in their consulting rooms. One of the most influential of these gurus was the cool, hyperpragmatic Jay Haley, family therapy’s most acerbic polemicist and the field’s closest link to the therapeutic lineage of the legendary hypnotherapist and master manipulator Milton Erickson. Rejecting the tradition of relationship-based psychotherapy as outdated and half-baked, Haley offered a vision of the clinician as a wily strategist and problem solver dedicated to finding the quickest, most efficient solution to the client’s difficulties, often circumventing the client’s best efforts to thwart the process.
In a 1982 Networker interview, Haley proclaimed in his characteristic tone of wry bemusement, “When people don’t know what to do in therapy, they become philosophers.” Skeptical of any therapy theory that sounded too fancy, he argued, “To be helpful to a therapist, a theory has to be simple enough so that it can help him think about what he actually needs to do with his clients.” Theories, he insisted, were usually more about why things stay the same than how to change them. “You might be able to understand what keeps a man drinking by looking at how his wife provokes him and see how she provokes him because he drinks. But it is very difficult to see in that description anything that helps you make an effective therapeutic intervention. . . . Being a therapist means not just looking at why things are what they are, but taking a position of responsibility about things being one way or another.”
In Haley’s view, it was the therapist’s job to make use of the inherent power of his position, without any nonsense about clinical neutrality or superfluous displays of empathy. There was a no-nonsense clarity and sense of both fierce commitment and emotional detachment in his unswerving focus on symptom alleviation that inspired many young therapists of the day. Part of his appeal may have been his preternatural calm, as if he inhabited a rarefied world beyond ordinary human strivings. If he ever had a sudden attack of countertransference, he hid it very, very well.
It’s hard to imagine a figure from that time more unlike Haley than the spontaneous and unpredictable Carl Whitaker, who embodied the kind of quirky authenticity celebrated in the human potential movement of the ’60s. Whitaker brought what he called his own “pseudocraziness” to his work, merrily ignoring all the usual rules and conventions of therapy in favor of what he believed should be a “nonverbal, shared fantasy experience.” Unlike Haley, he had no interest at all in his clients’ symptoms, and didn’t think it much mattered whether he “resolved” their problems or not. Like Haley, he rejected theory, but not out of pragmatism—he thought theory interfered with creative intuition, the ability to let his own unconscious somehow merge with the collective unconscious of the family he was treating. His “method” was an unscripted joyride of weird non sequiturs, off-the-wall challenges, gentle ridicule, and impossible directives (of the “be spontaneous” variety)—all presumably intended to access the secret labyrinth of the family’s unconscious life and the subterranean, unacknowledged fantasies family members shared about each other.
A rich vein of therapeutic folklore celebrating Whitaker’s zaniness and unflappability grew out of what he said and did, giving young therapists plenty of chance to ponder lessons not included in their grad school training. One story involved an irate, paranoid patient who once told Whitaker, “I’m going to get you and you’ll never know when it’s coming. One day, you may be standing at the urinal and a steel club will hit your head. What do you say to that?” To which Whitaker replied, without missing a beat, “Thanks for helping me. Up until now, all I had to worry about at the urinal was getting my shoe wet, but you’ve given me something else to think about.”
He cared not a fig about science or data, and would have been incredulous at today’s demands for therapists to meet empirical-validity standards. “I’m deliberately not interested in scientific rigor. . . . I would rather suffer for taking what I have and going full tilt with it than to be cautious and not get anywhere.” He certainly did not believe that he had any kind of world-changing destiny, as did some of the field’s crusaders—he just professed to do therapy because he couldn’t do anything else. For aspiring free spirits, he was the go-to role model of the day.
Perhaps nobody I interviewed had a greater sense of diva-like certitude or put on a more exhilarating show than Mara Selvini Palazzoli, leader of the Milan Team, a group of therapists whose work offered the purest expression of heady systems principles like “second order change” and “recursive loops.” Entering the family therapy field in the ’70s, her interventions offered deeply troubled families complex, double-level paradoxes warning them against the dangers of change. But then in the ’80s, she and her group switched and began issuing a series of “invariant prescriptions” or fixed directives. The most famous of these advised the parents to disappear from home for as short a time as three hours and as long as three months—without warning or explanation to their children. Since the families for whom this intervention was intended usually included a teenager diagnosed as “schizophrenic” (she tossed the word around with carefree abandon) or anorectic, the order threw families into an uproar. This was, of course, just the point—intended to break apart seriously dysfunctional coalitions between children and parents. Of course, it’s a form of intervention hard to even contemplate using in today’s far more litigious therapy world, but many were awestruck by the daring and intricacy of her procedures.
Listening to Palazzoli talk about her work was less like hearing someone describe the travails of a weekly caseload than like listening to an artist’s reflections on the evolution of her oeuvre. When asked whether it bothered her that she hadn’t stayed faithful to the model that had made her famous and had taken up with an even flashier one, she said grandly, “I am not interested in what I said 10 years ago. But this is typical for me because I have the tendency to despise everything I have already done and to be interested only in what I will do in the future.”
For many people, Virginia Satir was family therapy, the very embodiment of the optimistic, can-do spirit that launched the movement. The foremost woman among the field’s founding fathers, she seemed to tap effortlessly into people’s hidden emotion and turn the too-often stilted, diffuse rituals of therapy into exhilarating celebrations of people’s ability to transform their lives. You didn’t go just to listen to Virginia Satir present a workshop or interview a family. Even as you sat hidden in the anonymity of a large audience, she had a way of slipping past your guard and getting to you. Whether she was making you squirm by having you stare deeply into the eyes of the complete strangers sitting around you or just going on in that friendly, enormously reassuring voice about the untapped potential in every person, she refused to let you remain at arm’s length.
While others, like Haley and Palazzoli, approached the therapist’s task strategically and at a cerebral remove, Satir’s power was far more elemental, communicating an immediate sense of nurture that many found irresistible. In an early Networker interview she said, “When people come to see me, I don’t ask them if they want to change. I just assume they do. I don’t tell them what’s wrong with them or what they ought to do. I just offer my hand, literally and metaphorically. If I can convey to the person that I am trustworthy, then we can move and go to the scary places.”
No leader in the field seemed to communicate more of a sense of social mission than Salvador Minuchin, who also was recognized as family therapy’s most imitated maestro. In his work with poor families at the Wiltwyck School for Boys and later at the Philadelphia Child Guidance Clinic, he seemed to feel that his mandate went beyond therapeutic innovation to broader social change. Here’s how I described my first glimpse of him in a workshop I attended as a young therapist right out of grad school: “Standing in front of the audience of 200 therapists, Minuchin, a compact, dapper man with a Latin accent as thick as his black mustache, exuded an air of brusque command at odds with the traditionally pacifist culture of psychotherapy. Heaven protect anyone who stumbled through a lame question or tried to say a kind word about psychoanalysis. He seemed to me the most confident persona I had ever met, as if he had been to the mountaintop, seen the Truth and discovered he was It.”
In his clinical demonstrations, another persona emerged as well—a playful, charming, sleuth; a laid-back Inspector Poirot, taking in, as if by osmosis, every tiny clue that might help explain a family’s problems. More than any of his peers, with the possible exception of Satir, he transformed therapy into a kind of performance art. In a New Yorker profile, Janet Malcolm once described him this way: “Life is supposed to be disorderly, boring, fragmented, repetitive, in need of drastic editing. Watching a Minuchin session, or a tape of it, is like being at a tightly constructed, well-directed, magnificently acted play.”
For example, in one classic demonstration, he was working with a poor, black, single mother who couldn’t control her defiant 8-year-old son. After spending some time with the two, Minuchin asked the boy to stand up, saying, “I am still trying to figure out what makes you so powerful.” The boy stands up, grinning, and after complimenting him on how strong and healthy he looks, Minuchin asks the mother to stand up, too. As she towers over her small child, Minuchin asks, “Where did he get the idea that he is so powerful? He is a healthy boy, but look, he is just a little kid who somehow has convinced you that he is much older than he really is.” It was, I learned later, one of Minuchin’s favorite gambits, but as I watched it unfold, I was stunned by both the power and the sweetness of the moment. Both mother and son were smiling, basking in the attention they were receiving, coming more fully alive as if renewed by the prospect of order being restored in the family.
Later, under Minuchin’s gentle coaching, the mother finally was able to lay down some simple rules with some newfound authority in her voice. There was no doubt that she and her family had recorded a small victory in that room that day. I’m equally sure that over the next weeks and months, the therapists in that audience went on to direct hundreds of children and their parents through a similar routine, the image of Minuchin’s mastery still alive in their memories. Through family therapy’s formative years, he became the standard against which therapists measured their best work, and when they failed miserably or were confused about how to handle a case, they asked themselves what Minuchin might have done in the same situation.
Therapy’s Golden Age
While the early 1980s were a heady period for the entire field of psychotherapy, it was an even more exciting period for family therapy. Training institutes, clinical centers, and conferences popped up like daisies in early summer, while printing presses cranked out books and periodicals on systems theory and techniques with smoking speed. There was a sense that family therapy was part of an irresistible movement that would one day cure schizophrenia, defeat the slums, and resolve long-term depression and alcoholism in a few sessions! At times, it seemed as if psychotherapists had replaced the clergy as the wise, benevolent counselors of the era.
In short, the ’80s were a great time to begin publishing a therapy magazine chronicling the creative ferment and the cavalcade of clinical innovations. But as the decade progressed, it became more and more apparent that the journey to a therapy utopia wasn’t going to be such a smooth ride, nor without internal debate. Having originated in systems theory and a recognition of the broader society’s role in shaping human experience, the field kept exploring new perspectives that revealed the blind spots and limitations of its leaders. Among the field’s first and most influential critics were the Woman’s Project in Family Therapy, a group of outspoken feminists, who, by the later ’70s, had already begun to bring to the fore themes of female disempowerment that had been ignored by the profession’s largely male founders. As Networker Senior Editor Mary Sykes Wylie once wrote, the members of the Women’s Project were the first to articulate the cognitive dissonance many women in the field were experiencing, “a sense that family therapy techniques often resembled confidence tricks: within a framework of neutrality and equal respect for all, mothers were being had.” As Olga Silverstein, one of four Women’s Project’s members (the others being Betty Carter, Peggy Papp, and Marianne Walters), put it in a Networker interview, the family was “constituted so as to protect the patriarchal structure of society and the one-down position of women. The conventional family puts the male figure in the leadership role. The woman’s job is to serve. The better she serves, the better she is. If she doesn’t serve, it throws everything out of kilter.”
According to the feminists, the family therapy field itself had reconstituted a kind of professional patriarchy, with most of the power and authority in the field being held by men. Why did family therapy theory assume that the male and female roles in the family could be viewed in a social and political vacuum, without regard to the larger context that determined them? How was it that family therapy, which claimed to be so evenhanded, so often blamed the woman for whatever happened to the kids? Why did family therapists so often put pressure on the women in families to make the changes?
The feminist critique was just the first of a decade-long series of reexaminations of therapeutic practices and orthodoxies that the Networker published regularly through the ’80s, echoing changes in the broader culture. In magazine after magazine, we focused on topics and social issues not previously considered in the consulting room—race, domestic violence, social class, ethnicity—tackling subjects that most clinicians hadn’t thought relevant to their work. But in the increasingly psychologically attuned, tell-it-all ’80s, in which seeking therapy had become a kind of de rigueur new rite of passage, all sorts of once-taboo subjects were being addressed for the first time.
The lid to the Pandora’s Box of family secrets was literally exploding open, not just in therapy rooms, but in the recovery movement and self-help groups around the country. It was a Vesuvian eruption of revelations, touching on just about everything by everybody—alcoholism, drug addiction, infidelity, eating disorders, sex abuse, and incest. These formerly undiscussed subjects became a mainstay of People magazine and daytime TV. Phil Donahue, Oprah, and Sally Jesse Raphael shared the wealth with tens of millions of viewers. Psychotherapy had become a window on changes reverberating through society, and the Networker was in the thick of it.
If there was one secret revelation that overshadowed the others in the sense of shock and horror it evoked, it was surely the recognition of the widespread incidence of incest. Beginning in the late 1970s, the feminist movement made it possible for hundreds of thousands of women to share their long-hidden stories of childhood sexual abuse—and be believed. Soon thousands of women and men were telling the world about the traumatic sexual abuse perpetrated by their parents or other relatives. Commercial publishers quickly realized the potential marketing bonanza of this hot potato and books proliferated, filling whole sections of bookstores. It was both shocking and titillating to discover just how routine sexual abuse really was in even the “nicest,” most respectable families. A former Miss America revealed publicly that her father had sexually abused her for 13 years. The term “recovered memory” entered the popular lexicon, as did the name of a once-rare diagnosis, Multiple Personality Disorder, the presumed sufferers of which began to fill entire wards of psychiatric hospitals. The abuse chronicles reached a kind of dark apotheosis with the bizarre, widely broadcast tales not just of incest, but of satanic cults whose members used children in ritual acts of rape, torture, and murder.
With relatively little up-to-date research and almost no clinical tradition to rely on, therapists seeing these difficult cases were often flying by the seat of their pants. Many were essentially gob-smacked by the outpourings from their clients of terrible memories, images, and sensations of past abuse. The “excesses” of some therapists, as well as the sensationalized prosecutions and trials of parents accused of having years earlier abused their now-adult children, or taken part in grotesque satanic sex and death rituals, grabbed the headlines and the public’s attention, while steady, patient, careful work by mainstream therapists went unnoticed and unremarked. In March 1992, a group of parents protesting their own innocence of child-abuse charges formed a support and advocacy organization, the False Memory Syndrome Foundation. The foundation energetically targeted a large, amorphous “sex abuse industry,” including radical feminists, for fomenting general hysteria. More specifically, its members vented their fury at unethical, badly trained, credulous and/or manipulative therapists who used dodgy clinical techniques to elicit or pressure false disclosures of incest from essentially brainwashed clients. At the same time, psychotherapists who treated adult survivors found themselves defending their clinical integrity from what they often regarded as, at best, the reactive denial of accused parents, or at worst, a cynical, orchestrated attempt to once again suppress the truth about widespread child abuse.
In 1995’s “Caught in the Cross Fire,” Networker Features Editor Katy Butler captured the disorientation many clinicians were experiencing at “a time when old models can no longer explain new data and are being abandoned. And it had all the messiness that such shifts often entail. Some therapists believed every memory of satanic ritual abuse as gospel, passed around their own invented statistics, misused hypnosis, overdiagnosed, and drew heavily on self-help literature, autobiography, and pop psychology, borrowing checklists, insights, and simplistic dogmas from the addiction-recovery movement. If the influence of past abuse had gone unrecognized by the old paradigm, those involved in the new paradigm would focus on it to the exclusion of the present. . . . If earlier therapists had tacitly colluded with abusing fathers and mothers, they would now champion the daughters and sons. These were the excesses.”
But the critique of psychotherapy went beyond the repressed memory controversy and led Networker authors to focus not only on the field’s promise and potential for improving clients’ lives, but also on the harm that psychotherapy can do. Critics began to claim that the banalities of psychobabble and the “abuse excuse” were undermining individual responsibility. Psychotherapy, it was claimed, was creating a whiney culture of victimhood, which, instead of helping people acknowledge the past and then move on, was keeping them stuck in the victim role. Increasingly, as the decade progressed, those criticisms came not from outside the field, but from within it as well.
Commentators began discussing an imbalance afflicting the field that led many therapists to focus almost exclusively on their patients’ suffering, rather than their strengths and resilience—often encouraging the endless reliving of old trauma and reinforcing the survivors’ sense that they were deeply, perhaps irretrievably, wounded. As Laura Davis, coauthor of The Courage to Heal, the bible of the recovery movement, wrote in the Networker, “Eventually identifying only as a survivor is like wearing a sweater that is too small, and you need to take off, to stand up and say, ‘I am responsible for my own life, for what I do and what I am.’” Psychotherapist Dusty Miller, a survivor of child abuse herself, wrote, “The ripples that flow outward from every traumatic event don’t have to sink us, or assign us a single identity. ‘Victim,’ I want to tell them, describes a specific moment in time, not a permanent self-definition. This is a comforting aspect of the impermanence that transforms every emotional state.”
Following the Money
Our early focus as a publication had been on the intimate drama of the consulting room and the advances psychotherapy was making as a healing craft. But as the field grew and became more of a shaping force within the culture, it became harder to ignore the larger reality: mental healthcare was a multibillion dollar business. Much as we liked to view the profession with an almost bucolic innocence—as a loosely organized collection of friendly, well-meaning grocery store proprietors quietly tending their practices, in fact, large institutional players were reshaping the nature of the profession, determining what individual therapists could and couldn’t do and limiting the financial viability of their practices. Managed care’s relentless focus on cutting mental health reimbursements, the growing power of The Diagnostic and Statistical Manual of Mental Disorders, or DSM, and the increasing popularity of pharmaceuticals as alternatives to therapeutic treatment turned private practice from a comparatively easygoing, freewheeling, well-paid profession into a besieged enterprise struggling for economic survival. Much to their collective horror, therapists, largely a profession of refuseniks from the corporate world, were finding that, by and large, if they wanted to be paid for their work, they’d have to become entrepreneurs, make business plans, and worst of all, begin (gasp!) marketing themselves.
The 1994 publication of DSM–IV—a five-pound tome that included 340 different diagnoses—gave managed care companies a particularly effective screening tool for denying coverage. No longer could therapists just scribble in the code for “adjustment reaction”, the old DSM–III pro forma diagnosis and virtual free pass for insurance reimbursement. Now therapists without a readymade caseload had to take DSM seriously, parsing its definitions like Talmudic scholars if they wanted to get reimbursed. As one therapist said, “If DSM didn’t exist, managed care would have had to invent it.”
In hindsight, it was a devil’s bargain: therapists would play the diagnosing game as if the clients they saw suffered from “medical disorders,” treating them according to the equally fictitious “medical necessity,” and by so doing, be admitted into the medical club—at least long enough to get insurance reimbursement. The bargain worked well enough for many years, until managed care threw a wrench into the system by not only limiting reimbursement to specific diagnoses, but also accepting as “medically necessary” only those diagnoses that could be cured quickly. Treatment of choice (reimbursable treatment) often meant following officially established, short-term, “evidence-based treatment guidelines”—clear, manualized, unambiguous, reproducible recipes, intended to shorten and remove all ambiguity from the practice of therapy. So much for the Carl Whitaker school of treatment! Increasingly, a major ingredient in those recipes was medication. And more medication.
Following the enormous commercial success of the antidepressant Prozac, the ’90s ushered in what could be called the “era of the magic pill” with a tsunami of new psychotropic medications literally pouring forth as the drug companies rushed to get them to market. The Networker authors, while acknowledging the genuine usefulness of thoughtfully prescribed psychotropic drugs, were dismayed by the growing tendency toward pill pushing, not just in addition to, but instead of therapy. “The rising fascination with evolutionary psychology and biological determination has led some experts to proclaim, without much evidence, that all emotional states (including depression) are ultimately based on biology,” wrote clinical psychologist Michael Yapko in 1997. “But [the] devaluation of therapy that inevitably accompanies the new emphasis on biological approaches is wrongheaded on two fronts.” Not only did “epidemiological, social and cultural data indicate that, for most people, depression is not a disease of biological origin,” but “if, as the evidence now shows, cultural and social forces contribute more to the onset of depression than does biology, medication is only a partial solution. More important, there is now abundant evidence that therapy is as effective or more effective than drugs are for treating depression, with lower rates of relapse.”
In their prescient critique “Exposing the Mythmakers,” Barry Duncan, Scott Miller, and Jacqueline Sparks anticipated an avalanche of exposés of “Big Pharma” in the years to come, marshalling an impressive array of evidence that the hard sell for biomedical interventions was mostly hot air. “In all of the healing arts, there is no single explanation or simple, infallible remedy for any of the problems that beset humankind. Yet the growing power of the biological perspective in mental health discourse and practice suggests not only that there are solely biological explanations, but perfect, fail-safe biological solutions as well—simple pills that mark finis to everything from mild depression and nervous tension to panic attacks, bipolar disorder, and full-blown psychosis and schizophrenia.” How did this grossly simplistic and distorted view “come to hold almost unchallenged sway over both public and professional opinion? . . . Follow the money, and you will begin to understand the growth of the pharmaceutical behemoth.”
Widening the Lens
In 2001, the Networker officially acknowledged something that had been apparent to readers of the magazine for some time. Our coverage had shifted as the new ideas and clinical discoveries animating the field were no longer coming from family therapy or systems thinking. In fact, rather than the consulting room, much of the inspiration for new ways of approaching the therapist’s task was coming from nonclinicians in research labs. New developments in the broader scientific community were expanding the perspective of therapists and leading to the surprising conclusion that psychotherapy’s humanistic, relationship-oriented values weren’t at odds with the findings of modern science. In fact, researchers were legitimizing concepts and methods that had previously been on the margins of respectability and dismissed as “New Agey” and “touchy-feely.” More and more, the Networker was exploring topics like the nature of human emotion, mind–body approaches, mindfulness training, genetics and temperament, technology, and so on. Finally, it seemed only natural that the magazine’s name should better reflect the increasingly variegated material it contained. Thus, with the March/April issue, The Family Therapy Networker became the Psychotherapy Networker. We got some flak for “abandoning” family therapy, but as we saw it, we were just creating room for a bigger, more diverse “blended family” of therapeutic approaches, more attuned to the sprawling identity of the field as a whole.
Perhaps the most influential development of the past decade has been therapists’ increasing interest in brain science, which injected an unexpected but powerful jolt of “growth hormone” into our understanding of how and why therapy works. Freud had dreamed that someday therapists would understand the “neurology” behind psychopathology, but ever since, therapists had found it hard enough to focus on the mind and emotions, happily leaving the brain to its own mysterious devices.
There’s a tired, old quip people make when beginning a new undertaking that they think won’t be too difficult to learn or understand—“it’s not brain science.” Well, soon we were trying, in our limited way, to understand brain science, and the process was often excruciating. We began to discuss things like the neuroscience of emotion in the Networker, using new vocabulary, like the limbic system or emotional brain, and arguing that therapy didn’t always work well because it assumes that “our rational brains are in charge of our emotions, that what distinguished Homo sapiens from so-called ‘lower’ animals is our capacity to reason before we react,” as Brent Atkinson wrote in 1999, the culminating year of the Decade of the Brain. However, “our neural circuitry programs us instead to rage and cower and collapse in grief in a nanosecond, before we ever get a chance to fashion an ‘I’ statement or otherwise think things through.” In fact, Atkinson concluded, “our cerebral topography actually favors flaming emotionality, not sweet reason.”
Perhaps the most important new insight that therapists began to incorporate about the brain was that, as Mary Sykes Wylie wrote in “Discoveries from the Black Box” in 2002, our first issue devoted entirely to exploring the clinical implications of brain science, far from being a self-defining organ isolated inside our individual heads, “much brain function is an interpersonal phenomenon. Not only do brain structures and functions provide the means by which we connect with and make sense of one another, but through relational experience, parts of the brain, literally, grow. In fact, the brain, as we know it, is inconceivable without social relationships.” Successful psychotherapy is always and primarily a neurobiology-changing relationship. Furthermore, stories and narratives of the kind revealed in therapy—all those hours clients spend making sense of their raw, emotional experience—are “fundamental to brain function and attachment.”
According to psychiatrist Dan Siegel, who helped coin the term “interpersonal neurobiology” and as much as any contributor made understandable to therapists the brave new world of brain research revealed that, “Coherent stories are an integration of the left hemisphere’s drive to tell a logical story about events and the right brain’s ability to grasp emotionally the mental process of the people in those events. . . . Psychotherapy is perhaps the area where the human brain’s capacity for storytelling is most deeply engaged.” Finally, the brain is plastic: we develop new neural connections, and even develop new neurons in response to experience. In short, old-fashioned, nonscientific, nonmedical, and mostly not even “empirically validated” talk therapy was being restored to glory by the proponents of brain science, perhaps the most rigorous and certainly the most difficult of all the biological sciences—a satisfying, if paradoxical, development, indeed.
In no arena of practice did the interest in brain science have more impact than in trauma treatment, which previously had been seen by most therapists as a bad head trip, for which the standard approach was talk therapy of some kind, group support, and perhaps a Prozac prescription. But along with the expanding interest in understanding the human nervous system came the recognition that traumatized people continually relive trauma in mind, brain, and body, in physical sensations of frozen terror and helplessness—upset stomach, pounding heartbeat, sweaty hands, chest pressure, all signs of an autonomic nervous system run amok. Neuroimaging studies showed that when deeply traumatized people try to consciously access and put language to their trauma, their thinking brains essentially shut down, making them mostly unable to profit from standard talk therapy. As Bessel van der Kolk, a champion of a more somatically oriented approach to trauma, explained it, “The trauma doesn’t ‘sit’ in the verbal, understanding, part of the brain, but in much deeper regions of the brain—amygdala, hippocampus, hypothalamus, brain stem—which are only marginally affected by thinking and cognition. [P]eople process their trauma from the bottom up—body to mind—not top down,’” he added. “‘[T]o do effective therapy, we need to do things that change the way people regulate these core functions, which probably can’t be done by words and language.’” Taking the side of longtime body-oriented therapists, and basically blowing a raspberry at the research psychology establishment, van der Kolk argued that some form of body-based approach, whether EMDR, Somatic Experiencing, Sensorimotor Psychotherapy, or something else, was required before standard verbal therapy could get off the ground. Now, many of these interventions—so “fringy” when first introduced—as well as the thinking behind them, began to move into the mainstream.
It wasn’t only the scientific discoveries from brain science that were increasingly shaping psychotherapy’s direction. Impressive evidence from the growing new field of psychoneuroimmunology was demonstrating the powerful impact of mindfulness training on mental and physical health. Jon Kabat-Zinn, mindfulness practitioner and research scientist, began publishing studies that demonstrated that far beyond being merely a woo-woo New Age practice, meditation could make an enormous difference for people living with chronic pain and illness. Mindfulness training, he suggested in a 2004 Networker interview, could help people “cultivate intimacy” with their own bodies as standard medical or psychological approaches couldn’t. “Many of us are just really encapsulated in our head and in thought, while our bodies are kind of on their own,” he said. “Then when we experience pain or disease, we may realize that we’re actually in an adversarial relationship with our own body. When our body does something we don’t like—like come down with disease—we want to drive it to the hospital and have it fixed, as if it were an automobile.” Kabat-Zinn argued that meditation offers a means of giving people access to deep inner resources for healing “that are biologically available to all of us.”
A new model of practice, what Andrew Weil has called Integrative Mental Health, now has begun to take shape. In some ways, it’s a version of systems theory of 30 years ago, but instead of staying within the sphere of linear, left-brain understanding, it incorporates what we’ve learned about the relationships among mind, body, and spirit, along with our hard-won discoveries about how families and other social systems operate. Weil has quoted Albert Einstein to describe the connection between old and new knowledge in this emerging vision of mental healthcare: “Creating a new theory is not like destroying an old barn and erecting a skyscraper in its place. It is rather like climbing a mountain, gaining new and wider views, discovering unexpected connections between our starting point and its rich environment. But the point from which we started still exists and can be seen, although it appears smaller and forms a tiny part of our broad view gained by the mastery of the obstacles on our adventurous way up.”
The Conversation Ahead
So what lies ahead for psychotherapy and for this hardy little publication dedicated to telling the story of its continuing evolution? Like human beings and human history, therapy just keeps evolving and shape-shifting into forms we never can imagine ahead of time. When we began publishing this magazine, we were still entranced by the powerful voice of the family therapy revolutionaries. It did seem almost possible that they’d bring the bad old history of human unhappiness to an upbeat end and usher in a timeless era of psychological well-being. But over time, as we listened, different voices clamored for attention from different parts of the spectrum. These new conversations multiplied, overlapping and overriding each other, creating an unholy din at times. The upshot was that the answer to “What is good therapy?” didn’t grow simpler and more straightforward, but more complex—richer and more varied to be sure, but also more ambiguous.
The old top-down mode of conversation within our field is clearly a thing of the past. Since tapping into the worldwide community and the potential for instant communication through the Web, the potential for exchange within our field—the exponential increase in new voices, diverse ideas, ongoing arguments—seems almost unlimited. The question now is, How can we determine which voices, which conversations, will really contribute to psychotherapy’s store of genuine wisdom, and what can safely be dismissed as mere chatter?
Some years ago, after it had become glaringly obvious that we probably hadn’t discovered the single secret to human happiness after all, nor would we, I fastened on what became my favorite, catchall, security-blanket of a phrase, particularly useful in the face of facile truths, grandiose Big Ideas, or wildly popular fads. I discovered there’s hardly a case conference or a meeting about a Networker article or just about any occasion when it’s inappropriate to pause meaningfully, assume a wise look and say: “It’s more complicated than that.”
In fact, if editing this magazine has taught me anything about the multiple realities of human nature and the inherent difficulties of psychotherapy, it’s that, as a field, we must always be aware of our limitations, particularly when we’re broadcasting the latest, miraculous, one-size-fits-all model. That’s why it’s always important to listen to the critics along with the inventors of this or that fabulous new entry into the psychotherapy miracle-cure sweepstakes. Notice, I didn’t say we’d shun exciting new stuff. Who’d want to read us? But we always need to maintain a certain capacity for self-correction, which means, of course, always keeping the conversation going, no matter how loud and raucous it can sometimes get. In the meantime, given the endless variables of human beings and the infinite ways in which we can make ourselves miserable—and therefore in need of a good shrink—I wait for and wonder about what great new thing will bubble up next from the heaving collective consciousness of psychotherapy, and what will be found wanting about it.
As we step forward into the uncertain future of the field and this publication, I still take my guidance from Sal Minuchin, my first hero and today, at 90, still training young therapists and offering workshops around the world. According to him, no matter what the case he’s seeing or how much he continues to learn about what works in psychotherapy, one thing remains the same: “I’m always saying to people, in one way or another, ‘There are more possibilities in you than you think. Let us find a way to help you become less narrow.’” At another time, reflecting on the ups and downs of his own long career, he said, “I have failed in many ways, as most clinicians do. But when you fail, your certainty is transformed into questioning. I still see myself as an expert, but I know my truths are partial truths and my style of intervening is partial. Perhaps real wisdom is the uncertainty of the expert.”
Rich Simon
Richard Simon, PhD, founded Psychotherapy Networker and served as the editor for more than 40 years. He received every major magazine industry honor, including the National Magazine Award. Rich passed away November 2020, and we honor his memory and contributions to the field every day.






